Johns Hopkins University
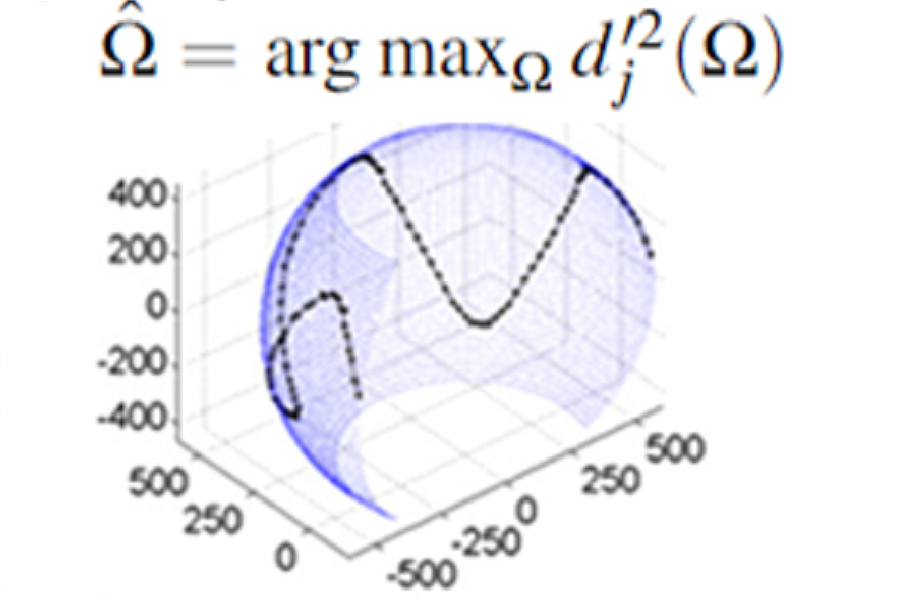
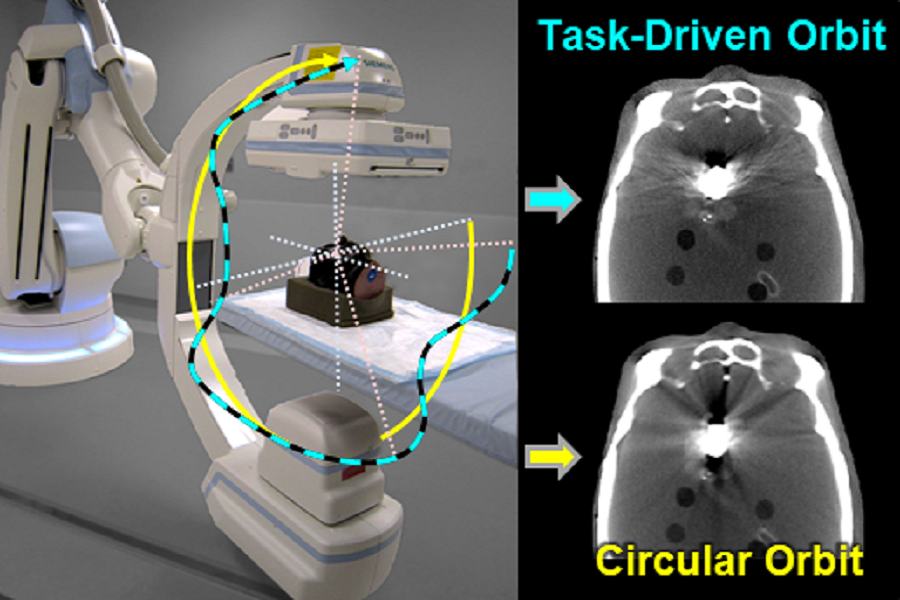
Task-driven source–detector trajectories in cone-beam computed tomography: II. Application to neuroradiology
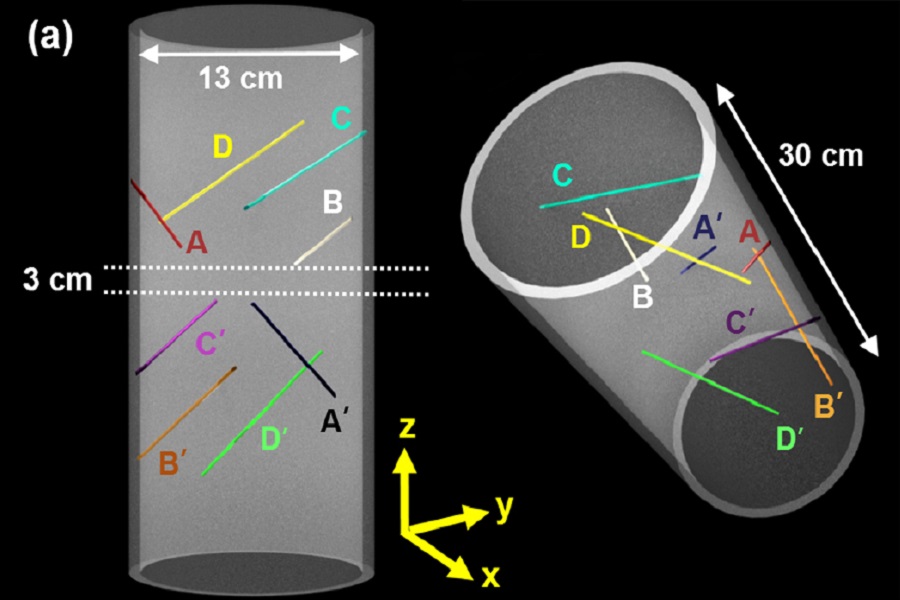
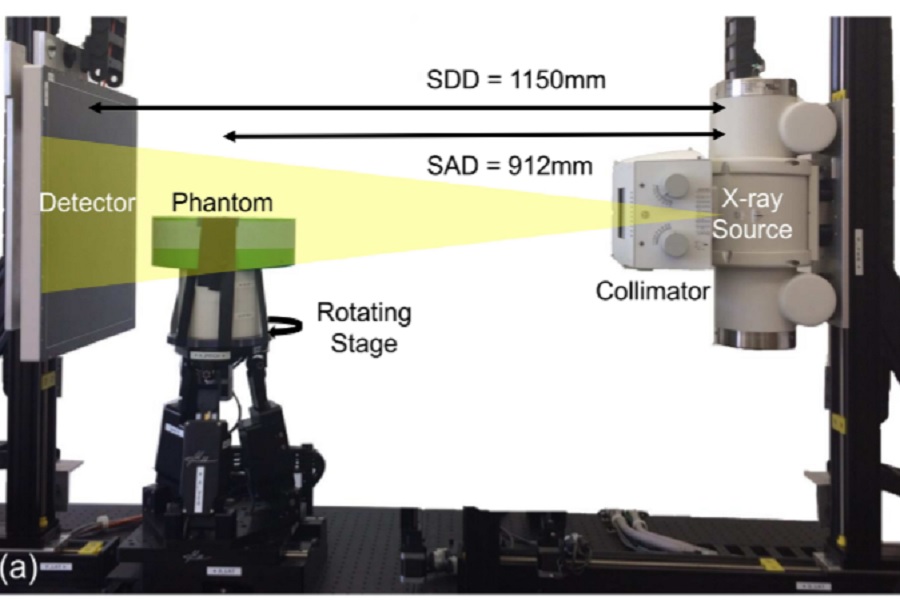
A line fiducial method for geometric calibration of cone-beam CT systems with diverse scan trajectories
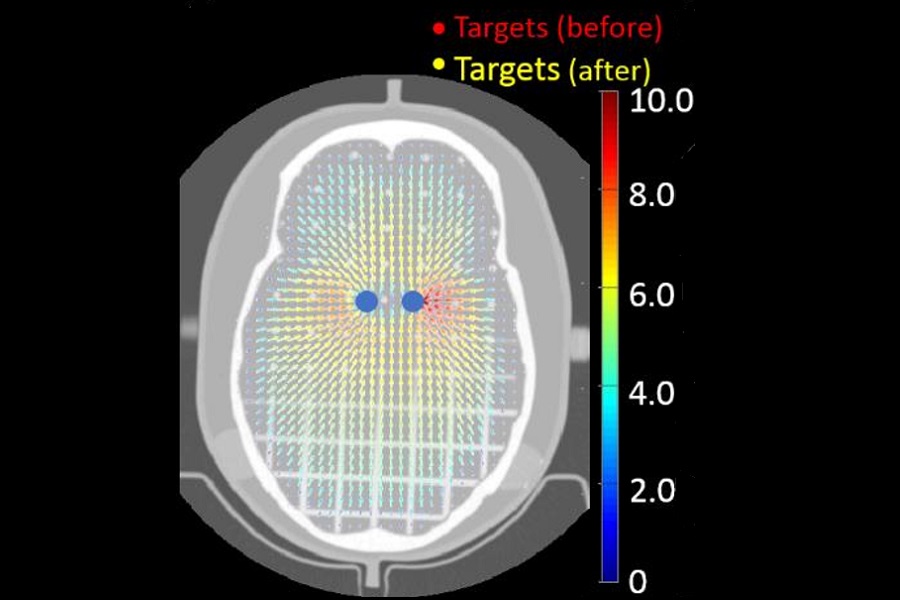
A Momentum-Based Diffeomorphic Demons Framework for Deformable MR-CT Image Registration
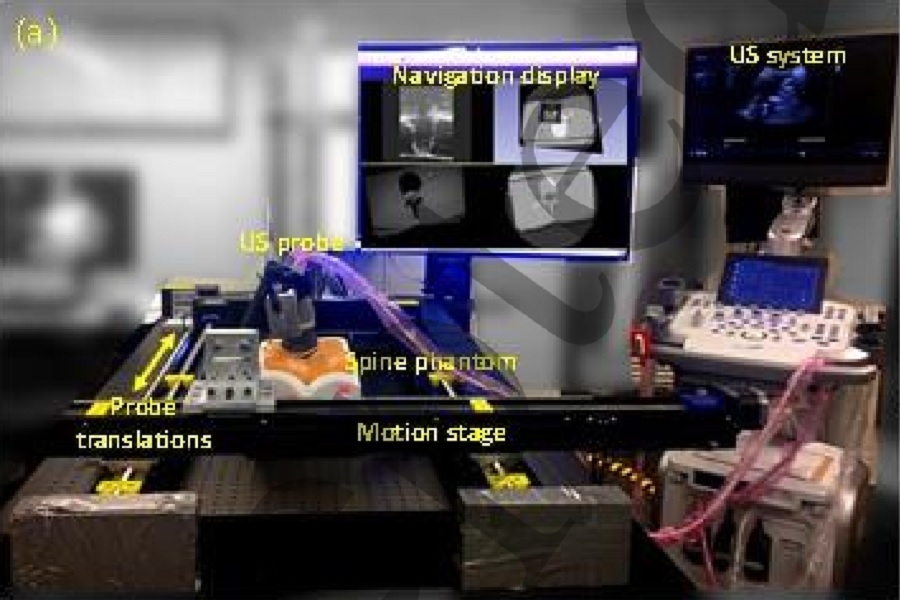
Real-time, image-based slice-to-volume registration for ultrasoundguided spinal intervention
Mobile C‐Arm with a CMOS Detector: Technical Assessment of Fluoroscopy and Cone‐Beam CT Imaging Performance
Predicting Image Properties in Penalized‐Likehood Reconstructions of Flat‐Panel CBCT
Image quality and dose characteristics for an O‐arm intraoperative imaging system with model‐based image reconstruction
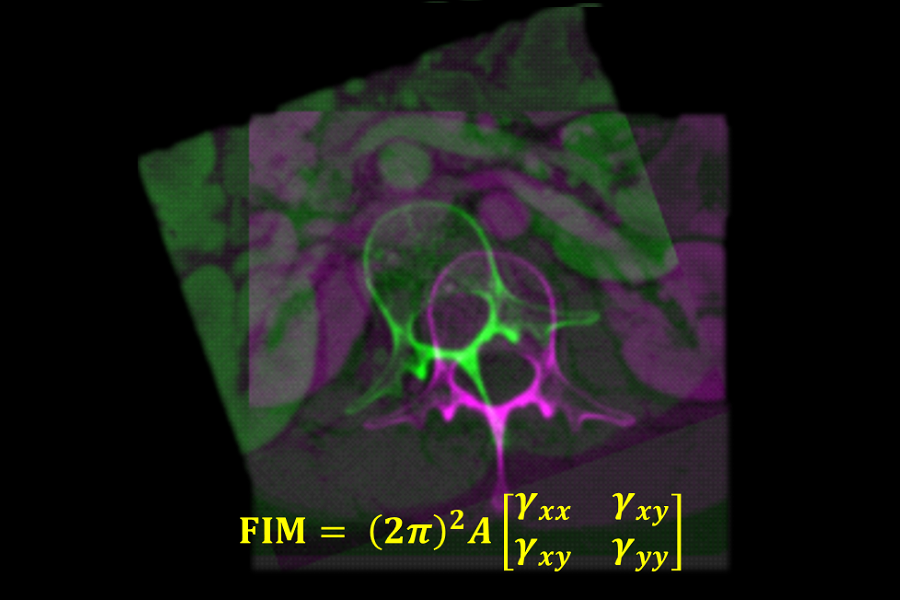
A Statistical model for rigid image registration performance: The influence of soft-tissue deformation as a confounding noise source
Automatic Planning and Guidance for Trauma Surgery – New Paper by Runze Han et al.
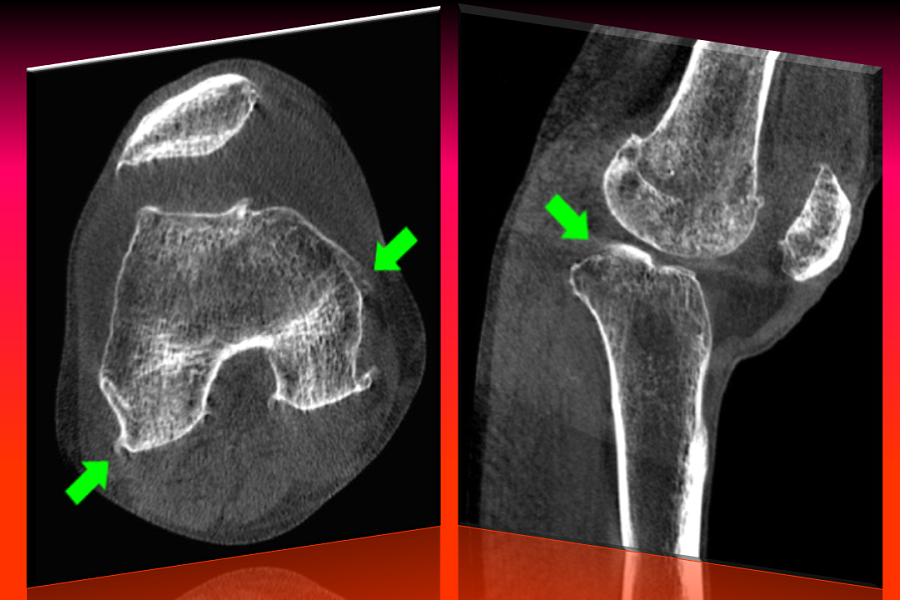
Motion compensation in extremity cone-beam computed tomography
Known‐component 3D image reconstruction for improved intraoperative imaging in spine surgery: A clinical pilot study
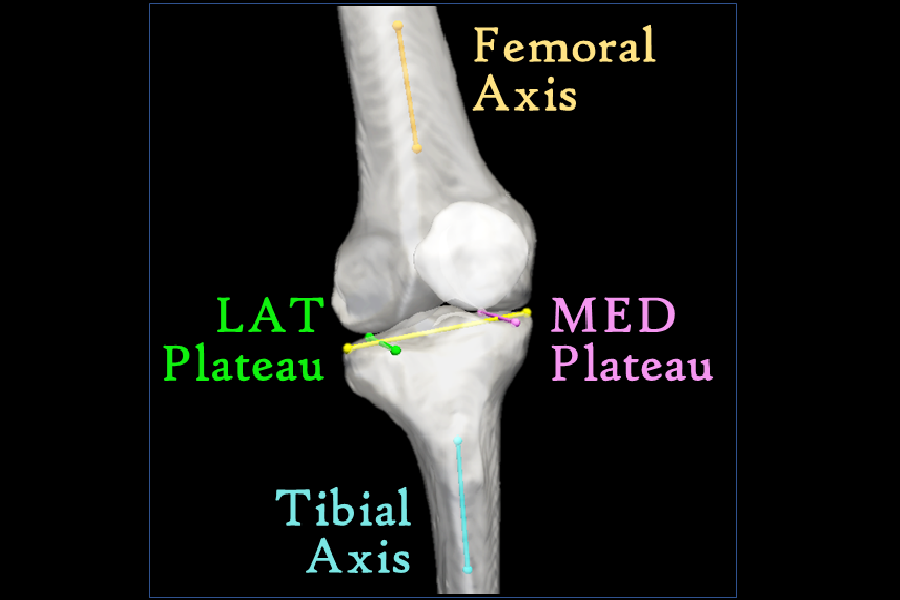
Atlas-based algorithm for automatic anatomical measurements in the knee
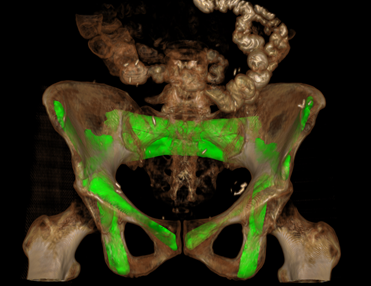
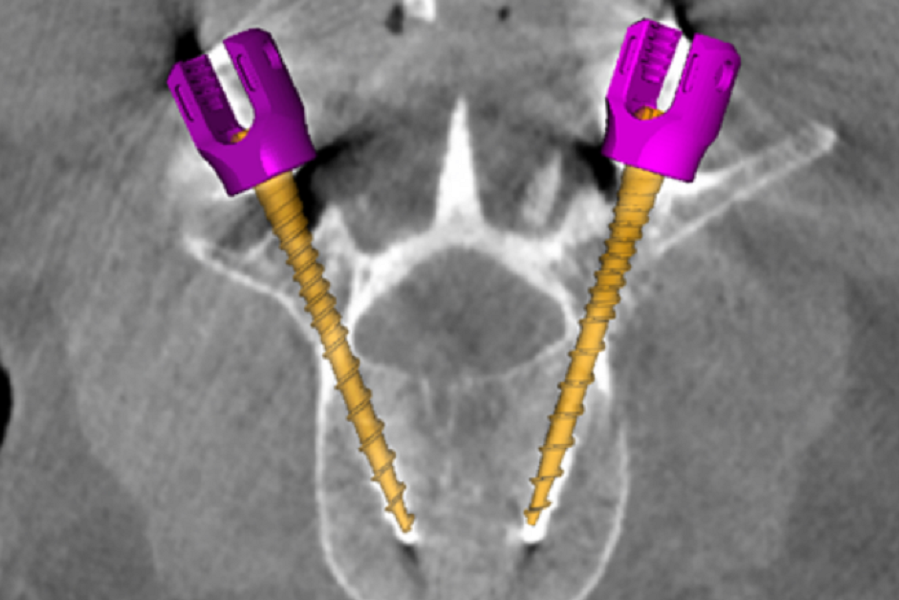
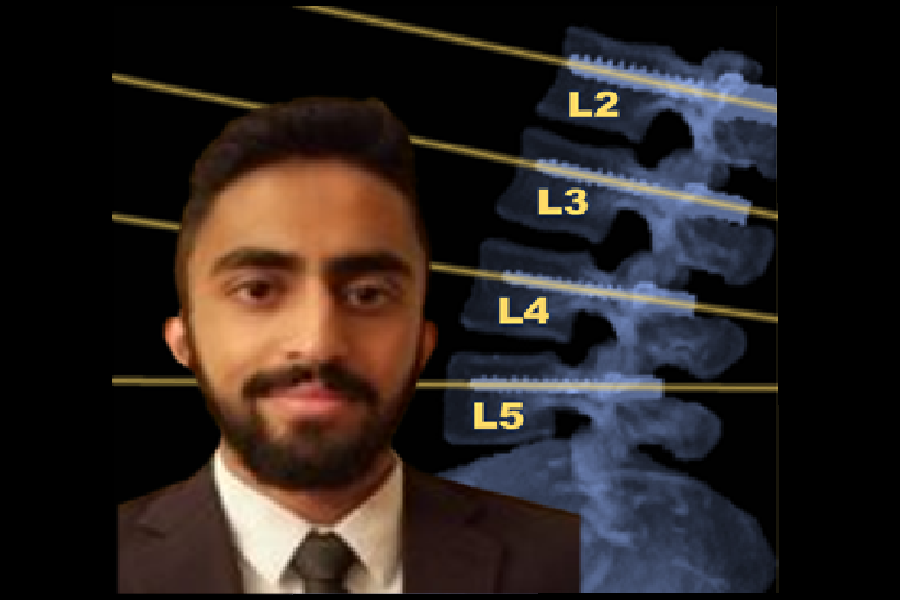
Automatic pedicle screw planning using atlas-based registration of anatomy and reference trajectories
Sorry, no publications matched your criteria.